…Writing a Different Story
NavigationCauses of Peroxisomal Disorders
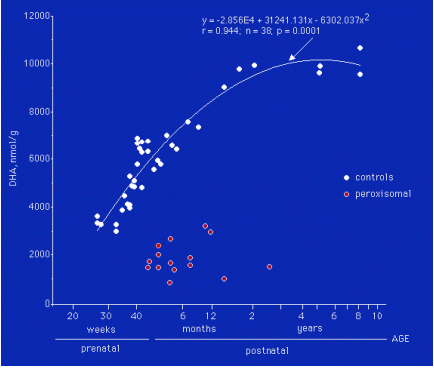
To date, there is no complete explanation on why peroxisomal disorders are so extremely severe. It is generally believed that the most damaging factor is the accumulation of the VLCFA 26:0 (a saturated fatty acid, with 26 carbon atoms and no double bonds) in the brain 4. However, this fatty acid is a normal constituent of myelin and, in the total forebrain, it rather decreases than increases following demyelination 5. Given the large concentration of plasmalogens in myelin, their decrease in peroxisomal disorders is a more plausible damaging factor in these patients. There is still another factor that could be the cause of much of the brain and visual damage, and this is the deficiency of docosahexaenoic acid (DHA), a most important polyunsaturated, omega-3 fatty acid (22:6ω3,6 double bonds and 22 carbon atoms) in the developing brain and retina. The DHA deficiency was discovered by M. Martinez in 1987, in the brain, liver, and kidneys of a Zellweger patient 6-8 and was confirmed later on in other patients with peroxisomal disorders 9-15. Fig. 1 shows the dramatic decreases in brain DHA found in 15 peroxisomal patients (red dots), compared to the normal developmental profile (white dots) in a logarithmic scale.
Since DHA is very important in neuronal synapses (connections between neurons) and in the photoreceptors (nerve cells specialized in vision) of the retina, much of the neurological and visual damage in these patients could be produced or, at least, aggravated by their DHA deficiency. This led M. Martinez to test whether the DHA deficiency could be corrected by exogenous administration of DHA and whether this could lead to some improvement of the clinical picture. The first patients were treated in 1992 16-18.